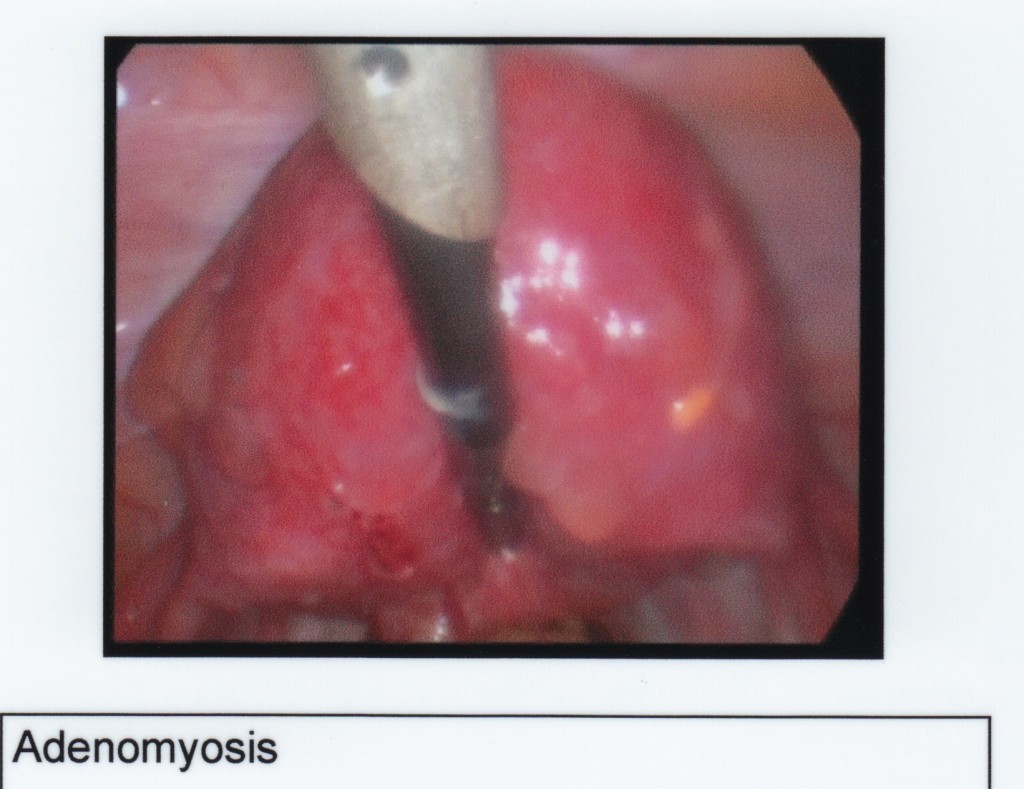
Adenomyosis is not endometriosis
Adenomyosis is very similar to endometriosis, in that it is the growth of the endometrium (uterine lining) where it should not be. Endometriosis grows on the surfaces in the pelvic region, and adenomyosis grows inside the muscle wall of the uterus. The endometrial tissue in both cases follows the menstrual cycle exactly as it does inside the uterus and bleeds during menstruation.
Important! If you ignore endometriosis it may develop into adenomyosis, which is much more difficult to treat.
Adenomyosis is a relatively uncommon condition. Although my surgeons say pre-menopausal women about the age of 40 suffer from it, they also say a huge number of cases are undiagnosed. Many menstruating women of all ages are simply putting up with the pain, heavy periods and infertility adenomyosis causes.
What happens when you have adenomyosis?
Adenomyomas (clumps of endometrial cells inside the wall of the uterus) bleed, creating pockets of blood, very much like the swelling and bad bruise that appears after a sprain. Because this pool of blood is inside the muscle, the muscle fibres can’t respond and contract properly to control the menstrual flow. This results in very heavy period bleeding with many large blood clots.
My surgeon once described this muscle reaction as “like trying to spit through a mouthful of marbles” - you’ll lose a lot more fluid than if you could simply spit without the marbles.
This tissue doesn’t start bleeding a couple of days in advance of a period like endometriosis does, but the pools of blood inside the uterus wall in the adnomyomas cause increasingly more pain towards the end of the menstrual cycle.
Adenomyosis can cause infertility and more often miscarriages, as it is a growth inside the walls that disrupts the tissue supporting the growing fetus.
What causes it?
As with most of the pelvic diseases, there are no known causes. Unfortunately, not much research has been done as it mostly affects older women, and is usually fully removed with a hysterectomy. Less is known about adenomyosis than endometriosis, although the two seem to be related.
Adenomyosis often occurs alongside other diseases, most commonly with endometriosis and irritable bowel syndrome (IBS). Fibroids, cysts, and other pelvic diseases are common co-morbidities.
How do you detect adenomyosis?
For endometriosis, fibroid and adenomyosis patients, the gold standard is a biopsy, followed by internal ultrasounds and MRIs to diagnose the presence and extent of the abnormal endometrial and fibroid growths.
It’s likely that you will be diagnosed with adenomyosis when everything else is ruled out.
Biopsy during laparoscopy or after hysterectomy
The most reliable detection of ademonyosis is with a biopsy of the removed uterus after a hysterectomy. The surgeons and pathologists can take their time and thoroughly test all areas of the muscle.
Experienced surgeons may take punch biopsies of the uterus wall wherever it looks boggy, swollen, lumpy and not smooth. This is commonly done at the same time as a laparoscopy to identify and remove endometriosis lesions, fibroids or cysts.
Imaging for adenomyosis
One other diagnosis method that has a decent chance of success of detecting the abnormal tissue inside the uterine wall is an MRI. Unfortunately, most health insurers around the world won’t cover this test for suspected adenomyosis.
One other common method of initial diagnosis is using ultrasound to check the size of the uterus. The uterus may (or may not) ‘swell’ and enlarge with the scar tissue and blood inside the muscle wall. Often sufferers will talk about a ‘4 week size uterus’ - comparing the size of their enlarged uterus with the size of a pregnant woman’s uterus. If the adenomyosis is advanced, black areas that look like cysts may appear inside the muscle wall.
Ultrasound technology has been substantially improved with doppler readings to show blood flow. Adenomyomas have abnormal blood flow, and more advanced growths can be detected with this method. Trained radiologists should know what to look for.
Of course, you need to time these tests with your period. Once the period ends, the blood will be slowly reabsorbed into the body as a ‘waste product’.
CA125 blood test
The CA125 blood test is actually a cancer indicator that specialists sometimes use to detect endometriosis. Unfortunately, it is extremely unreliable. Inflamed or damaged ovaries, fallopian tubes, uterus, cervix and the lining of the abdominal cavities and chest all release Cancer Antigen 125.
For someone who has never had cancer, the average level is under 35. If you have cancer, the level would be at least 1500. With endometriosis, fibroid and adenomyosis, the CA125 level may be around 80, but is a very imprecise. More often, doctors will use this test to monitor endometriosis after diagnosis. The results may go up as the endometriosis grows, and down on removal.
Endometriosis, fibroids, pelvic infections, liver disease and adenomyosis can all raise CA125 levels. Too many false positive results means this test is not a useful indication of ovarian cancer. However, cancer patients can use it to monitor their CA125 levels while undergoing treatment and afterwards.
From personal experience, the CA125 test misses positive cases too. I had severe adenomyosis throughout the entirety of the uterine muscle, but my CA-125 levels were essentially normal
CA125 controversy
Unfortunately, a chain-email encourages women to insist on a yearly CA125 test as an early detection method for ovarian cancer. This test is terribly unreliable, with results differing from patient to patient. CA125 can not definitively indicate the presence or absence of cancer. Snopes.com discusses the chain-email in detail, with comments from cancer centres and doctors.
How do you treat adenomyosis?
The preferred method of treatment for older women is a partial or full hysterectomy. This removes 100% of the adenomyosis growths, and will have an immediate pain relieving effect. Of course, there are risks with hysterectomies - infections, nerve damage, prolapsed bladder, bowel problems. Consider these before you make a decision.
If you don’t have endometriosis, a partial hysterectomy or endometrial ablation may fully get rid of the disease and the symptoms. As it doesn’t remove the ovaries, you will not experience the hormonal change to menopause.
A hysterectomy is a big operation. Make sure you plan your recovery - you may need to take it easy for quite some time, especially if you have other chronic illnesses. I think it was a good six months after my partial laparoscopic hysterectomy before I felt fit enough for normal activity levels.
Treating endometriosis and adenomyosis together
If you have endometriosis as well, a partial hysterectomy will not provide full pain relief. The endometriosis will still bleed into the pelvic cavity every cycle, triggered by the hormones released by the ovaries. Even if you have a laparoscopy to remove the endometriosis lesions, they will likely regrow. A full hysterectomy may provide more relief, as this puts the body into menopause.
There are downsides to doing this too early though - especially the bone loss leading to osteoporosis. You can use hormone replacement therapy (HRT) to mask the nastier effects of menopause that some women can experience. Unfortunately, HRT contains oestrogen which will continue to feed the endometriosis growths inside the pelvis.
If you are close to menopause when adenomyosis is finally diagnosed, you may find a hysterectomy to be your best option. If you have developed adenomyosis at a much younger age, the choice of treatments is far from ideal.
Treatments in younger women
To put off more drastic methods, you can stop the bleeding with the Mirena intra-uterine device (IUD), or the Visanne progestin tablet. Both methods are reversible at any time.
A trial of Mirena on adenomyosis sufferers found that it decreased the severity and in some cases removed the symptoms entirely. It does not treat the adenomyomas (growths) at all, but delivers a low dose of progesterone directly into the uterus lining, slowing and sometimes stopping the growth of the lining (and thus periods). It seems to be more effective than the continuous pill as there seem to be much fewer side effects.
Gynecologists should replace the Mirena IUD every 4-5 years as the amount of hormones released into the uterus decreases over time. The implant procedure is definitely not painless - I would personally recommend using an anaesthetic.
Using endometriosis medications such as continuous high progesterone birth control (BCP), or the newer medication Visanne (progestin), may control the growth rate of the adenomyomas and the pain by avoiding periods. Although, Visanne may have some nasty side-effects.
Even if you have a Mirena IUD, if you also have endometriosis, many doctors will recommend you stay on a very low dose pill or Visanne in addition to stop the action of the ovaries.